While I know full well that this is not my usual type of post, I've copied and pasted a lot of great information here for folks who may be experiencing the signs of afib. These signs should be taken seriously. As for experiencing Atrial fibrillation, also known as "afib," it can be scary. I'm posting the information below to provide you, my readers, with information in an effort to help you if you're experiencing the symptoms of this.
During atrial fibrillation, the heart's two upper chambers (the atria) beat chaotically and irregularly — out of coordination with the two lower chambers (the ventricles) of the heart. Atrial fibrillation symptoms often include heart palpitations, shortness of breath and weakness.
Episodes of atrial fibrillation may come and go, or you may develop atrial fibrillation that doesn't go away and may require treatment. Although atrial fibrillation itself usually isn't life-threatening, it is a serious medical condition that sometimes requires emergency treatment.
A major concern with atrial fibrillation is the potential to develop blood clots within the upper chambers of the heart. These blood clots forming in the heart may circulate to other organs and lead to blocked blood flow (ischemia).
Treatments for atrial fibrillation may include medications and other interventions to try to alter the heart's electrical system.
Symptoms:
- Some people with atrial fibrillation have no symptoms and are unaware of their condition until it's discovered during a physical examination. Those who do have atrial fibrillation symptoms may experience signs and symptoms such as:
- Palpitations, which are sensations of a racing, uncomfortable, irregular heartbeat or a flip-flopping in your chest
- Weakness
- Reduced ability to exercise
- Fatigue
- Lightheadedness
- Dizziness
- Shortness of breath
- Chest pain
- Occasional. In this case it's called paroxysmal (par-ok-SIZ-mul) atrial fibrillation. You may have symptoms that come and go, usually lasting for a few minutes to hours. Sometimes symptoms occur for as long as a week and episodes can happen repeatedly. Your symptoms might go away on their own or you may need treatment.
- Persistent. With this type of atrial fibrillation, your heart rhythm doesn't go back to normal on its own. If you have persistent atrial fibrillation, you'll need treatment such as an electrical shock or medications in order to restore your heart rhythm.
- Long-standing persistent. This type of atrial fibrillation is continuous and lasts longer than 12 months.
- Permanent. In this type of atrial fibrillation, the abnormal heart rhythm can't be restored. You'll have atrial fibrillation permanently, and you'll often require medications to control your heart rate and to prevent blood clots.
If you have any symptoms of atrial fibrillation, make an appointment with your doctor. Your doctor may order an electrocardiogram to determine if your symptoms are related to atrial fibrillation or another heart rhythm disorder (arrhythmia).
If you have chest pain, seek emergency medical assistance immediately. Chest pain could signal that you're having a heart attack.
Causes
Atrial fibrillation
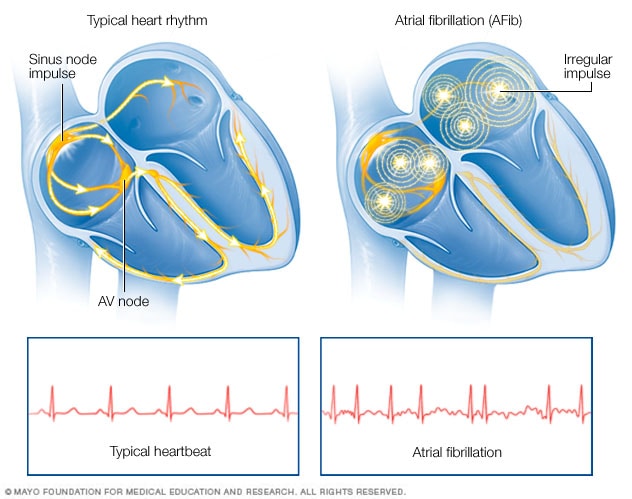
Atrial fibrillation is an irregular and often rapid heart rate that occurs when the two upper chambers of your heart experience chaotic electrical signals. The result is a fast and irregular heart rhythm. The heart rate in atrial fibrillation may range from 100 to 175 beats a minute. The normal range for a heart rate is 60 to 100 beats a minute.
Your heart is made up of four chambers — two upper chambers (atria) and two lower chambers (ventricles). Within the upper right chamber of your heart (right atrium) is a group of cells called the sinus node. This is your heart's natural pacemaker. The sinus node produces the signal that normally starts each heartbeat.
Normally, the signal travels through the two upper heart chambers, and then through a connecting pathway between the upper and lower chambers called the atrioventricular (AV) node. The movement of the signal causes your heart to squeeze (contract), sending blood to your heart and body.
In atrial fibrillation, the signals in the upper chambers of your heart are chaotic. As a result, they quiver. The AV node — the electrical connection between the atria and the ventricles — is bombarded with impulses trying to get through to the ventricles.
The ventricles also beat rapidly, but not as rapidly as the atria, as not all the impulses get through.
Possible causes of atrial fibrillation:
- Abnormalities or damage to the heart's structure are the most common cause of atrial fibrillation. Possible causes of atrial fibrillation include:
- High blood pressure
- Heart attack
- Coronary artery disease
- Abnormal heart valves
- Heart defects you're born with (congenital)
- An overactive thyroid gland or other metabolic imbalance
- Exposure to stimulants, such as medications, caffeine, tobacco or alcohol
- Sick sinus syndrome — improper functioning of the heart's natural pacemaker
- Lung diseases
- Previous heart surgery
- Viral infections
- Stress due to surgery, pneumonia or other illnesses
- Sleep apnea
Atrial flutter
Atrial flutter is similar to atrial fibrillation, but the rhythm in your atria is more organized and less chaotic than the abnormal patterns common with atrial fibrillation. Sometimes you may have atrial flutter that develops into atrial fibrillation and vice versa.
The risk factors for and the symptoms and causes of atrial flutter are similar to those of atrial fibrillation. For example, strokes are also a concern in someone with atrial flutter. As with atrial fibrillation, atrial flutter is usually not life-threatening when it's properly treated.
Risk factors
Certain factors may increase your risk of developing atrial fibrillation. These include:
- Age. The older you are, the greater your risk of developing atrial fibrillation.
- Heart disease. Anyone with heart disease — such as heart valve problems, congenital heart disease, congestive heart failure, coronary artery disease, or a history of heart attack or heart surgery — has an increased risk of atrial fibrillation.
- High blood pressure. Having high blood pressure, especially if it's not well-controlled with lifestyle changes or medications, can increase your risk of atrial fibrillation.
- Other chronic conditions. People with certain chronic conditions such as thyroid problems, sleep apnea, metabolic syndrome, diabetes, chronic kidney disease or lung disease have an increased risk of atrial fibrillation.
- Drinking alcohol. For some people, drinking alcohol can trigger an episode of atrial fibrillation. Binge drinking may put you at an even higher risk.
- Obesity. People who are obese are at higher risk of developing atrial fibrillation.
- Family history. An increased risk of atrial fibrillation is present in some families.
- Complications
- Stroke. In atrial fibrillation, the chaotic rhythm may cause blood to pool in your heart's upper chambers (atria) and form clots. If a blood clot forms, it could dislodge from your heart and travel to your brain. There it might block blood flow, causing a stroke.
- Heart failure. Atrial fibrillation, especially if not controlled, may weaken the heart and lead to heart failure — a condition in which your heart can't circulate enough blood to meet your body's needs.
Prevention:
- To prevent atrial fibrillation, it's important to live a heart-healthy lifestyle to reduce your risk of heart disease. A healthy lifestyle may include:
- Eating a heart-healthy diet
- Increasing your physical activity
- Avoiding smoking
- Maintaining a healthy weight
- Limiting or avoiding caffeine and alcohol
- Reducing stress, as intense stress and anger can cause heart rhythm problems
- Using over-the-counter medications with caution, as some cold and cough medications contain stimulants that may trigger a rapid heartbeat
To diagnose atrial fibrillation, your doctor may review your signs and symptoms, review your medical history, and conduct a physical examination. Your doctor may order several tests to diagnose your condition, including:
- Electrocardiogram (ECG). An ECG uses small sensors (electrodes) attached to your chest and arms to sense and record electrical signals as they travel through your heart. This test is a primary tool for diagnosing atrial fibrillation.
- Holter monitor. This portable ECG device is carried in your pocket or worn on a belt or shoulder strap. It records your heart's activity for 24 hours or longer, which provides your doctor with a prolonged look at your heart rhythms.
- Event recorder. This portable ECG device is intended to monitor your heart activity over a few weeks to a few months. When you experience symptoms of a fast heart rate, you push a button, and an ECG strip of the preceding few minutes and following few minutes is recorded. This permits your doctor to determine your heart rhythm at the time of your symptoms.
- Echocardiogram. This test uses sound waves to create moving pictures of your heart. Usually, a wandlike device (transducer) is held on your chest. Sometimes, a flexible tube with the transducer is guided down your throat through to your esophagus. Your doctor may use an echocardiogram to diagnose structural heart disease or blood clots in the heart.
- Blood tests. These help your doctor rule out thyroid problems or other substances in your blood that may lead to atrial fibrillation.
- Stress test. Also called exercise testing, stress testing involves running tests on your heart while you're exercising.
- Chest X-ray. X-ray images help your doctor see the condition of your lungs and heart. Your doctor can also use an X-ray to diagnose conditions other than atrial fibrillation that may explain your signs and symptoms.
- The atrial fibrillation treatment that is most appropriate for you will depend on how long you've had atrial fibrillation, how bothersome your symptoms are and the underlying cause of your atrial fibrillation. Generally, the treatment goals for atrial fibrillation are to:
- Reset the rhythm or control the rate
- Prevent blood clots, which may decrease the risk of a stroke
In some people, a specific event or an underlying condition, such as a thyroid disorder, may trigger atrial fibrillation. Treating the condition causing atrial fibrillation may help relieve your heart rhythm problems. If your symptoms are bothersome or if this is your first episode of atrial fibrillation, your doctor may attempt to reset the rhythm.
Resetting your heart's rhythm
Ideally, to treat atrial fibrillation, the heart rate and rhythm are reset to normal. To correct your condition, doctors may be able to reset your heart to its regular rhythm (sinus rhythm) using a procedure called cardioversion, depending on the underlying cause of atrial fibrillation and how long you've had it.
Cardioversion can be done in two ways:
- Electrical cardioversion. In this brief procedure, an electrical shock is delivered to your heart through paddles or patches placed on your chest. The shock stops your heart's electrical activity for a short moment. The goal is to reset your heart's normal rhythm.
- Cardioversion with drugs. This form of cardioversion uses medications called anti-arrhythmics to help restore normal sinus rhythm. Depending on your heart condition, you may receive medications through an IV or by mouth to help return your heart to normal rhythm.
Before cardioversion, you may be given warfarin or another blood-thinning medication for several weeks to reduce the risk of blood clots and strokes. If your episode of atrial fibrillation lasted more than 48 hours, you may need to take this type of medication for at least a month after the procedure to prevent blood clots in the heart.
Maintaining a normal heart rhythm:
After electrical cardioversion, your doctor may prescribe anti-arrhythmic medications to help prevent future episodes of atrial fibrillation. Medications may include:
- Dofetilide
- Flecainide
- Propafenone
- Amiodarone
- Sotalol
- Nausea
- Dizziness
- Fatigue
Heart rate control
You may be prescribed medications to control how fast your heart beats and restore it to a normal rate.
You may be prescribed medications to control how fast your heart beats and restore it to a normal rate.
Digoxin.
This medication may control the heart rate at rest, but not as well during activity. Most people need additional or alternative medications, such as calcium channel blockers or beta blockers.
Beta blockers. These medications can help to slow the heart rate at rest and during activity. They may cause side effects such as low blood pressure (hypotension).
Beta blockers. These medications can help to slow the heart rate at rest and during activity. They may cause side effects such as low blood pressure (hypotension).
Calcium channel blockers.
These medicines also can control your heart rate, but may need to be avoided if you have heart failure or low blood pressure.
Catheter and surgical procedures
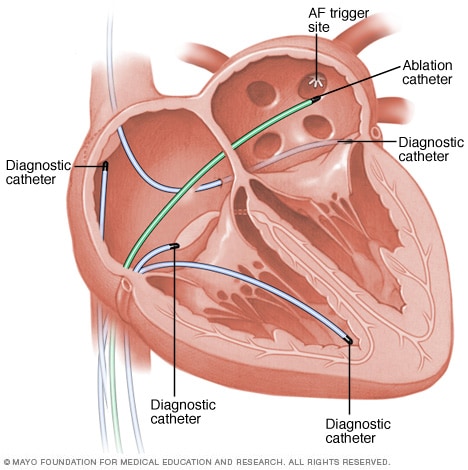
Catheter ablation to isolate the pulmonary veins to treat atrial fibrillation
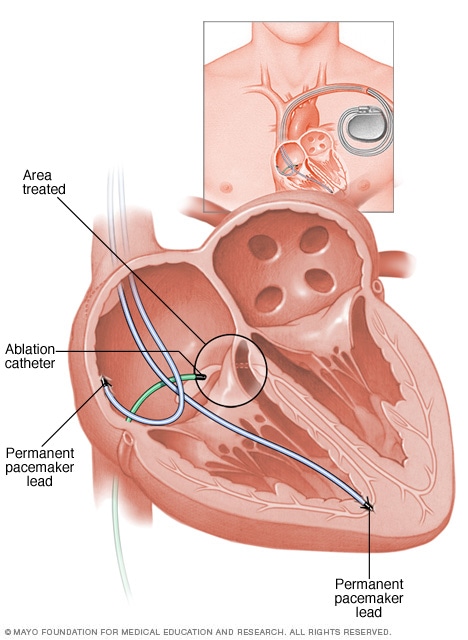
AV node ablation
Sometimes medications or cardioversion to control atrial fibrillation doesn't work. In those cases, your doctor may recommend a procedure to destroy the area of heart tissue that's causing the erratic electrical signals and restore your heart to a normal rhythm. These options can include:
Catheter ablation. During this procedure, a doctor inserts long, thin tubes (catheters) into your groin and guides them through blood vessels to your heart. The catheter's tip produces radiofrequency energy, extreme cold (cryotherapy) or heat to destroy areas of heart tissue that are causing rapid and irregular heartbeats. Scar tissue forms, which helps signaling return to normal. Cardiac ablation may correct the arrhythmia without the need for medications or implantable devices.
Your doctor may recommend this procedure if you have atrial fibrillation and an otherwise normal heart and medication has not improved your symptoms. It may also be helpful for heart failure patients who have an implanted device and cannot take or tolerate anti-arrhythmic medications.
Maze procedure.
There are several variations of the maze procedure. The doctor may use a scalpel, radiofrequency or extreme cold (cryotherapy) to create a pattern of scar tissue that interferes with stray electrical impulses that cause atrial fibrillation.
The maze procedures have a high success rate, but atrial fibrillation may come back. If this happens, you may need another cardiac ablation or other heart treatment.
Because the surgical maze procedure (using a scalpel) requires open-heart surgery, it's generally reserved for people who don't get better with other treatments or when it can be done during a necessary heart surgery, such as coronary artery bypass surgery or heart valve repair.
Atrioventricular (AV) node ablation. If medications or other forms of catheter ablation don't work or cause side effects, or if you're not a good candidate for these therapies, AV node ablation may be an option. The procedure involves using a catheter to deliver radiofrequency energy to the pathway (AV node) connecting the upper and lower heart chambers.
The procedure destroys a small area of heart tissue, preventing abnormal signaling. However, the upper chambers of the heart (atria) will still quiver. You'll need a pacemaker to be implanted to keep the lower chambers (ventricles) beating properly. You'll need to take blood thinners after this procedure to reduce the risk of a stroke due to atrial fibrillation.
Preventing blood clots
Many people with atrial fibrillation or those who are undergoing certain treatments for atrial fibrillation are at especially high risk of blood clots that can lead to a stroke. The risk is even higher if other heart disease is present along with atrial fibrillation.
Anticoagulants
Your doctor may prescribe blood-thinning medications (anticoagulants) such as:
Many people have spells of atrial fibrillation and don't even know it — so you may need lifelong anticoagulants even after your rhythm has been restored to normal.
Left atrial appendage closure
Your doctor may also consider a procedure called left atrial appendage closure.
In this procedure, doctors insert a catheter through a vein in the leg and eventually guide it to the upper left heart chamber (left atrium). A device called a left atrial appendage closure device is then inserted through the catheter to close a small sac (appendage) in the left atrium.
This may reduce the risk of blood clots in certain people with atrial fibrillation, as many blood clots that occur in atrial fibrillation form in the left atrial appendage. Candidates for this procedure may include those who don't have heart valve problems, who have an increased risk of blood clots and bleeding, and who are aren't able to take anticoagulants. Your doctor will evaluate you and determine if you're a candidate for the procedure.
Lifestyle and home remedies
You may need to make lifestyle changes that improve the overall health of your heart, especially to prevent or treat conditions such as high blood pressure and heart disease. Your doctor may suggest several lifestyle changes, including:
If you think you may have atrial fibrillation, it is critical that you make an appointment with your family doctor. If atrial fibrillation is found early, your treatment may be easier and more effective. However, you may be referred to a doctor trained in heart conditions (cardiologist).
Because appointments can be brief, and because there's often a lot to discuss, it's a good idea to be prepared for your appointment. Here's some information to help you get ready for your appointment, and what to expect from your doctor.
The maze procedures have a high success rate, but atrial fibrillation may come back. If this happens, you may need another cardiac ablation or other heart treatment.
Because the surgical maze procedure (using a scalpel) requires open-heart surgery, it's generally reserved for people who don't get better with other treatments or when it can be done during a necessary heart surgery, such as coronary artery bypass surgery or heart valve repair.
Atrioventricular (AV) node ablation. If medications or other forms of catheter ablation don't work or cause side effects, or if you're not a good candidate for these therapies, AV node ablation may be an option. The procedure involves using a catheter to deliver radiofrequency energy to the pathway (AV node) connecting the upper and lower heart chambers.
The procedure destroys a small area of heart tissue, preventing abnormal signaling. However, the upper chambers of the heart (atria) will still quiver. You'll need a pacemaker to be implanted to keep the lower chambers (ventricles) beating properly. You'll need to take blood thinners after this procedure to reduce the risk of a stroke due to atrial fibrillation.
Preventing blood clots
Many people with atrial fibrillation or those who are undergoing certain treatments for atrial fibrillation are at especially high risk of blood clots that can lead to a stroke. The risk is even higher if other heart disease is present along with atrial fibrillation.
Anticoagulants
Your doctor may prescribe blood-thinning medications (anticoagulants) such as:
- Warfarin. Warfarin may be prescribed to prevent blood clots. If you're prescribed warfarin, carefully follow your doctor's instructions. Warfarin is a powerful medication that may cause dangerous bleeding. You'll need to have regular blood tests to monitor warfarin's effects.
- Newer anticoagulants. Several newer blood-thinning medications (anticoagulants) are available to prevent strokes in people with atrial fibrillation. These medications include dabigatran, rivaroxaban, apixaban and edoxaban. They are shorter acting than warfarin and usually don't require regular blood tests or monitoring by your doctor. These medications aren't approved for people who have mechanical heart valves.
Many people have spells of atrial fibrillation and don't even know it — so you may need lifelong anticoagulants even after your rhythm has been restored to normal.
Left atrial appendage closure
Your doctor may also consider a procedure called left atrial appendage closure.
In this procedure, doctors insert a catheter through a vein in the leg and eventually guide it to the upper left heart chamber (left atrium). A device called a left atrial appendage closure device is then inserted through the catheter to close a small sac (appendage) in the left atrium.
This may reduce the risk of blood clots in certain people with atrial fibrillation, as many blood clots that occur in atrial fibrillation form in the left atrial appendage. Candidates for this procedure may include those who don't have heart valve problems, who have an increased risk of blood clots and bleeding, and who are aren't able to take anticoagulants. Your doctor will evaluate you and determine if you're a candidate for the procedure.
Lifestyle and home remedies
You may need to make lifestyle changes that improve the overall health of your heart, especially to prevent or treat conditions such as high blood pressure and heart disease. Your doctor may suggest several lifestyle changes, including:
- Eat heart-healthy foods. Eat a healthy diet that's low in salt and solid fats and rich in fruits, vegetables and whole grains.
- Exercise regularly. Exercise daily and increase your physical activity.
- Quit smoking. If you smoke and can't quit on your own, talk to your doctor about strategies or programs to help you break a smoking habit.
- Maintain a healthy weight. Being overweight increases your risk of developing heart disease. Healthy weight loss can help to manage symptoms of atrial fibrillation and may improve the results of catheter ablation.
- Keep blood pressure and cholesterol levels under control. Make lifestyle changes and take medications as prescribed to correct high blood pressure (hypertension) or high cholesterol.
- Drink alcohol in moderation. Binge drinking (having five drinks in two hours for men or four drinks for women) can increase your chances of atrial fibrillation. In some people, even modest amounts of alcohol can trigger atrial fibrillation.
- Maintain follow-up care. Take your medications as prescribed and have regular follow-up appointments with your doctor. Tell your doctor if your symptoms worsen.
If you think you may have atrial fibrillation, it is critical that you make an appointment with your family doctor. If atrial fibrillation is found early, your treatment may be easier and more effective. However, you may be referred to a doctor trained in heart conditions (cardiologist).
Because appointments can be brief, and because there's often a lot to discuss, it's a good idea to be prepared for your appointment. Here's some information to help you get ready for your appointment, and what to expect from your doctor.
What you can do
- Be aware of any pre-appointment restrictions. At the time you make the appointment, be sure to ask if there's anything you need to do in advance, such as restrict your dietary intake. You may need to do this if your doctor orders blood tests.
- Write down any symptoms you're experiencing, including any that may seem unrelated to atrial fibrillation.
- Write down key personal information, including any family history of heart disease, stroke, high blood pressure or diabetes, and any major stresses or recent life changes.
- Make a list of all medications, vitamins or supplements that you're taking.
- Take a family member or friend along, if possible. Sometimes it can be difficult to understand and remember all the information provided to you during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your doctor.
For atrial fibrillation, some basic questions to ask your doctor include:
- What is likely causing my symptoms or condition?
- What are other possible causes for my symptoms or condition?
- What kinds of tests will I need?
- What's the most appropriate treatment?
- What foods should I eat or avoid?
- What's an appropriate level of physical activity?
- How often should I be screened for heart disease or other complications of atrial fibrillation?
- What are the alternatives to the primary approach that you're suggesting?
- I have other health conditions. How can I best manage them together?
- Are there any restrictions that I need to follow?
- Should I see a specialist? What will that cost, and will my insurance cover seeing a specialist? (You may need to ask your insurance provider directly for information about coverage.)
- Is there a generic alternative to the medicine you're prescribing?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend visiting?
What to expect from your doctor
- Your doctor is likely to ask you a number of questions. Being ready to answer them may save time to go over any points you want to spend more time on. Your doctor may ask:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- What, if anything, seems to improve your symptoms?
- What, if anything, appears to worsen your symptoms?
If you are experiencing Afib, any of the signs and symptoms, please get checked.
Tom Correa